Introduction
Endodontic retreatment has a predictable success rate in the hand of experienced operator.[1] Removal of the obturation material from the root canal system can be achieved by a variety of techniques. The removal is often complicated by presence of separated instruments, posts, ledges or canal blockade. Endodontic retreatment will be successful only if all the material in the root canal is removed and obturation with bacteria impervious seal is obtained in the apical region following thorough cleaning and shaping.
Endodontic posts are often used to retain the core for a full coverage restoration in a mutilated tooth which has lost most of its coronal tooth structure. Custom cast, prefabricated metal and prefabricated fiber posts are frequently used and all gives good success rate. In case of endodontic failure, removal of the endodontic post is often a complicated procedure with probability for unsuccessful removal, perforation of the root, partial removal, weakening of the root structure and root fracture.[2],[3] The removal procedure is more complicated if the endodontic post is fractured as the apical segment is far from the orifice to see, appreciate and remove. Removal of threaded endodontic post is complicated by the presence of threads engaging the dentinal surface with increased retention. This paper reports a case of mandibular premolar with a fractured threaded metal endodontic post which was removed successfully with masserrann instrument retrieval kit and restored with ribbond reinforced endodontic post and esthetic crown restoration.
Case Report
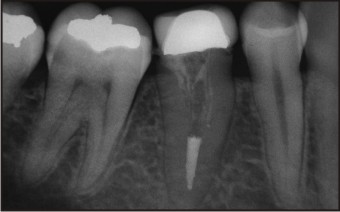
A male patient, 20 years old reported to Department of Conservative Dentistry and Endodontics with the chief complaint of food lodgment and bleeding from gingiva in the right back teeth region. Clinical examination revealed a full metal crown with overhanging margins on mandibular right second premolar (45) and secondary caries in the distal proximal gingival margin of the tooth, under the crown, (Figure 1). Intraoral periapical (IOPA) radiograph of the tooth revealed a fractured endodontic post and the coronal fragment was malaligned compared to the apical part and the root canal obturation was not satisfactory (Figure 2). It was decided to remove the metal crown and excavate the secondary caries, remove the fractured post, reobturate the apical third of the root canal, fabricate a ribbond post and core and finally replace the metal crown with an esthetic crown.
 | Figure 1. Full metal crown with bulbous gingival margins are seen.
 |
 | Figure 2. IOPA radiograph reveals over contoured crown and fractured endodontic post.
|
Full metal crown was removed with crown remover. Secondary caries on the distal margin was excavated with round carbide bur in a slow speed hand-piece. Using a round diamond point, the tip of the coronal fragment was exposed. Then using a tapered fissure diamond point a narrow slot was made around the fractured post and was retrieved by holding with narrow artery forceps. In order to gain access to the apical segment, the canal was widened with number 3 gates glidden drill. With a thin tapered fissure bur, a narrow slot was prepared around the post. Ultrasonic vibrations were used to dislodge the post in counter clockwise direction to the threads. The tip of the post was narrowed by cutting the threads in the most coronal portion to engage the masserann instrument removal kit. Once it was engaged, rotating in the counter clockwise direction, the fractured segment was removed(Fig 3). The remaining root canal obturation material was removed using H-Files and Endosolv (gutta percha solvent). Working length was determined, cleaning and shaping was performed and sectional obturation was done using gutta percha as obturation material and AH Plus as sealer.
 | Figure 3. Coronal and apical fractured endodontic post removed.
|
Patient was advised for oral prophylaxis and the same was done next day. Patient was recalled after 5 days.
Clinical examination of the root canal revealed oval shaped canal that was wide and irregular. So it was decided to restore and reinforce the root with ribbond (Poly ethylene fiber) and make a composite core. 3 mm wide ribbond fiber of about 20 mm length was taken and folded. It was moistened in adper single bond 2 (Bonding agent).The canal was etched with 37% phosphoric acid, bonded with adper single bond 2 and flooded with flowable composite. The folded end was placed inside the canal and the free ends were placed coronally. Light curing was done with high intensity LED (light emitting diode) light curing unit (Elipar, 3M ESPE) for 1 minute to ensure complete polymerization of the composite. Core build-up was done with composite resin (Filtez Z-350) and tooth preparation for porcelain fused to metal (PFM) crown was made. PFM crown was fabricated and cemented in the subsequent visit (Fig 4). IOPA radiograph was taken to check the marginal adaptation and contour of the cemented crown (Figure 5).
 | Figure 4. PFM crown cemented and healthy free gingival margin seen.
|
 | Figure 5. IOPA radiograph reveals proper marginal adaptation and proximal contour.
|
Discussion
The goal of ideal root canal treatment is not only to clean, shape and obturate the root canal space but to restore the mutilated tooth back to its proper form, function and esthetics. Apart from the operators effort, there are chances of endodontic mishaps that could adversely affect the treatment outcome. In case of endodontic treatment failure, retreatment could be performed orthrograde (from the coronal aspect) or retrograde by endodontic surgery. It is preferable to choose orthograde treatment if previous orthograde treatment was not performed, the cause for failure could be treated orthograde with a expected predicatable success rate. In this case orthograde treatment was selected because of the presence of secondary caries in the margin and ill fitting metal crown which mandatorily dictates the removal of crown, close proximity of tooth root to mental foramen and mandibular canal and improper root canal obturation.
The purpose of endodontic post is to provide retention to the core and distribute the occlusal load uniformly along the root surface. Torbjorner et al[4] reported on the frequency of three technical failures (loss of retention, root fracture, and post fracture). Post fracture alone contributes least to the failure of restoration, but the distribution of forces may become uneven and eventually root fracture may result.
In the present case ultrasonics and masserann kit was used for the removal of the fractured post as ultrasonics is the easiest, reliable technique with fewer incidences of root fracture and perforations.[5] The threaded post poses serious difficulties as they are engaged deeply inside the dentine. So masserann instrument removal kit was used to hold the fractured segment and to retrieve it.[6],[7]
Polyethylene fiber has shown to reinforce the weakened root structures. In this case pre fabricated post was not selected because the canal anatomy was oval and irregular. The prefabricated post which are round in cross section and the weakened root structure contraindicate the use of custom cast post and core.[8] It is difficult to identify ribbond (Poly ethylene fiber) in radiograph because of their radio-lucent nature so care should be taken while placement. The core build-up was done with direct composite as it is compatible with ribbond fibers.
By replacing with a properly contoured crown, the normal health of the gingiva was maintained. Tooth coloured porcelain fused to metal crown enhanced the esthetic value also.
Conclusion
If performed with utmost care, restoring a mutilated tooth back to function is time consuming but, possible. Ultrasonics remains as the best technique for removal of endodontic post. Placement of ribbond fiber to reinforce the root and restore coronal tooth structure seems to be ideal, less time consuming and reliable treatment.
References
1. Torabinejad M, Corr R, Handysides R, Shabahang S. Outcomes of nonsurgical retreatment and endodontic surgery: a systematic review. J Endod. 2009;35:930-7.
2. Castrisos T, Abbott PV. A survey of methods used for post removal in specialist endodontic practice. Int Endod J. 2002;35:172-80.
3. Abbott PV. Incidence of root fractures and methods used for post removal. Int Endod J. 2002;35:63-7.
4. Torbjorner A, Karlsson S, Odman PA. survival rate and failure characteristics for two post designs. J Prosthet Dent 1995;73:439-44.
5. Plotino G, Pameijer CH, Grande NM, Somma F. Ultrasonics in endodontics: a review of the literature. J Endod. 2007;33:81-95.
6. Gencoglu N, Helvacioglu D. Comparison of the different techniques to remove fractured endodontic instruments from root canal systems. Eur J Dent. 2009;3:90-5.
7. Yoldas O, Oztunc H, Tinaz C, Alparslan N. Perforation risks associated with the use of Masserann endodontic kit drills in mandibular molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;97:513-7.
8. Kimmel SS. Restoration of endodontically treated tooth containing wide or flared canal. N Y State Dent J. 2000;66:36-40.
|